

Hearing Care

Causes of Hearing Loss
There are 3 basic types of hearing loss: sensorineural, conductive and mixed
Sensorineural Hearing Loss – results from damage to the inner ear or hearing nerve (cochlea).
Causes of sensorineural hearing loss include:
- Aging – gradual age-related hearing loss called presbycusis
- Prolonged exposure to loud noises
- Viral or bacterial infections of the ear
- Certain medications and antibiotics
- Meniere’s Disease
- Acoustic Neuroma – a tumor which is located in the ear
- Hereditary factors
Conductive Hearing Loss – occurs when sound is not conducted efficiently through the ear canal, ear drum or middle ear
Causes of conductive hearing loss include:
- Infection of the ear canal or middle ear
- Fluid in the middle ear
- Perforation or scarring of the eardrum
- Wax build-up
- Dislocation of the ossicles (the three middle-ear bones)
- Foreign objects in the ear canal
- Otosclerosis – an abnormal growth of bone near the middle ear
- Unusual growths, tumors
Mixed Hearing Loss – occurs when there is a combination of both sensorineural and conductive issues, when both the middle ear and inner ear are affected.
Symptoms of Hearing Loss
Because it happens gradually, hearing loss often goes unnoticed. Denial is a common occurrence. Here are some common signs of hearing loss:
- speaking louder than necessary in conversation
- constantly asking for words to be repeated
- straining to hear
- misunderstanding conversations, especially in noisy situations
- favouring one ear
- thinking that people always mumble
- turning the television or radio up louder than usual
- having difficulty hearing on the telephone
- withdrawing from social contact
- ringing or buzzing in one or both ears
- appearing dull and disinterested, slow to respond, or passive and detached
The impact of hearing loss on older adults
- With unmanaged hearing loss, older adults may become withdrawn and socially isolated which can lead to the breakdown of support networks and the risk of depression.
- Older adults with unmanaged hearing loss are at an increased risk of cognitive decline and developing Alzheimer’s disease and other forms of dementia. However, there is encouraging evidence that hearing assistance, such as a hearing aid, can improve the lives of even those with significant dementia.
- Research has revealed that there is a greater risk of falling with hearing loss, and the risk of falling increases with the severity of the hearing loss.
- 90% of people with hearing loss can improve communication with a properly fitted hearing aid, counselling or environmental changes.
If you are experiencing any of these signs of hearing loss, it is important to obtain a hearing test and proper treatment when necessary.


Hearing Aids
About Hearing Aids
A hearing aid is a small electronic device that is worn in or behind a person’s ear. It processes sounds and amplifies them so that they are audible for a person with hearing loss. In the past, hearing aids focused primarily on enhancing communication, but modern hearing aids focuses on improving the quality of listening in individuals, whereby providing comfortable listening. Statistics show that ninety percent of the people with hearing loss benefits greatly from the use of hearing aids.
As technology advances, hearing aids are changing both in size and quality. Digital programmability of hearing aids have made them extremely versatile and enabled fitting to a wide range of patients depending on their degree and type of hearing loss.
Parts of a Hearing Aid
Functionally, hearing aid can be divided into three blocks: 1. The microphone 2. The amplifier and, 3. The receiver or speaker. The microphone picks up the incoming sound and sends it to the amplifier circuit. The amplifier processes the signal and feeds it to the receiver. The receiver transmits the processed sound into the ear of the user.
Even though the location of structures varies from manufacturer to manufacturer, basic external features are shared by most hearing aids. They include Microphones, On-Off switch, Battery compartment, the volume control, program selection switch, connection tube/ear hook/ear tip and the dome/ear mold or receiver. To reduce the size of hearing aids, sometimes the on-off switch is designed to work as volume switches or programming switch depending on the duration of pressing the button

Different types of hearing aids
Hearing aids can be broadly classified into two main groups: in-the-ear (ITE) styles and behind-the-ear (BTE) styles.
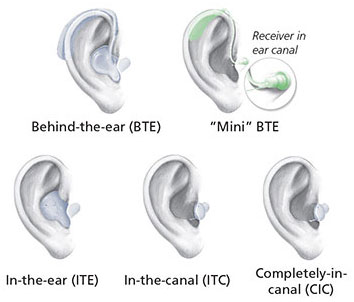
ITE styles
Invisible-in-the-canal (IIC) and completely-in-the-canal (CIC) hearing aids are the smallest hearing aids to date. They fit very deeply in the ear canal and are typically fit for mild or moderate hearing losses. Their size and ability to “disappear” when worn depend on the size of the ear canal. Because of their tiny size, they offer high cosmetic appeal for people who desire a discreet solution.
In-the-canal (ITC) hearing aids sit in the lower portion of the concha part of the external ear, making them comfortable and easy to use. Because they are slightly larger than IIC and CIC styles, they have a longer battery life, are easier to handle and can fit a wider range of hearing losses.
BTE styles
Behind-the-ear hearing aids, as their name suggests, are worn behind the pinna of the user. The sound is carried to the ear canal by a very thin ear tubes and an ear tip that fade discreetly into the ear canal. They have enough physical space to house features for a variety of hearing losses. Owing to the larger form factor, these hearing aids have easy to manipulate manual controls and longer lasting batteries. For higher degrees of hearing loss, ear molds have to be used to prevent the leakage of amplified sound from the ear canal of the user.
Mini BTE hearing aids with slim tubes and tips: Mini BTE styles are designed to hide behind the outer ear and have ultra-thin tubing to discreetly route sound into the ear. This style is so popular that a greater variety of ear tips have become available in order to accommodate a greater degree of hearing loss with the mini BTE.
Receiver-in-the-ear (RITE) or receiver-in-canal (RIC) hearing aids: RITE and RIC styles have the receiver (speaker) built into the ear tip instead of the main body of the hearing aid. This allows the speaker of the hearing aid to be positioned closer to the eardrum while the microphone and processor sit in a tiny case behind the ear.
Professionals involved in Hearing Aid fitting
The professionals involved in Hearing Aid fitting and prescriptions are the Audiologist and the Hearing Instrument Practitioners. A health care professional who is trained to evaluate hearing loss and related disorders, including balance (vestibular) disorders and tinnitus (ringing in the ears) and to rehabilitate individuals with hearing loss and related disorders. A Hearing instrument practitioner/specialist is a professional trained to handle various types of hearing aids and assistive listening devices.
Care and Maintenance of Hearing Aid
Hearing aids are electronic devices with many sensitive components. Hence it is of utmost importance to treat the hearing aid with care in order for it to function longer and minimize potential problems during daily use. Hearing aids are often robust but they may not be able to withstand long periods of abuse.
It is important to keep the hearing aid away from dirt and moisture. Making sure that hands are clean and dry before touching the hearing aid is a good way to prevent the clogging of the small microphone inlet.
Removing hearing aids before showering, swimming or during the rain prevents moisture from entering the device. It is generally advised to clean the hearing aids every day with a dry cloth and keep the device in dehumidifier boxes over night to ensure longevity of the device.
Keep the hearing aids away from pets and avoid exposing them to hair spray. When hearing aids are not used for a while, remove the batteries and keep them separate from the aid.
Never attempt to open the casing or repair the hearing aids. The circuit of hearing aids is very sensitive to static electricity and may be irreversibly damaged by any attempt to open the casing.
Adapting to Hearing aids – The learning curve
One should never expect to hear as good as normal ears as soon as one is fitted with a hearing aid. There is a learning curve associated with the usage and adaptation to hearing aids. The people who lose their hearing gradually and the people who do not treat hearing loss for a long time have difficulty adapting to the hearing aids. The lack of listening to sounds for a long time may have made them sensitive to environmental sounds and when the hearing aid quickly lets them hear these sounds, the sensation may be overwhelming and distracting at first. Hence, the hearing care specialist provides the hearing aid user with a daily schedule to use the hearing aid till the person is comfortable with using the device for long periods of time.
Tinnitus
What is tinnitus?
Tinnitus is a problem that affects about 10% to 15% of the population. It is often described as a ringing, buzzing or pulsating sound in the ear, but is defined as a phantom auditory sound (i.e. perceived sound in the absence of an external noise). Many people who suffer from tinnitus also experience tension in their head, neck and jaw, tiredness, irritability, poor concentration, anxiety and depression that can be severe. About 5% of the population reports severely intrusive tinnitus affecting day-to-day activities.
What causes tinnitus?
Most cases of chronic tinnitus are thought to be a result of damage to the microscopic nerve endings in the inner ear. However, current research now suggests that a more central region of the brain (i.e. dorsal cochlear nucleus) has been identified as a potential culprit especially when it is accompanied with a loss of hearing (i.e. auditory input reduction). Tinnitus is a symptom and not a disease and is often the result of an injury to the peripheral auditory system, hearing nerve and/or auditory centres in the brain. Wax buildup, eardrum perforation, ear infection, barotitis (i.e. ear blockage after a flight), noise exposure, advancing age, head injury, teeth grinding, intense period of stress, certain medications (i.e. aspirin in high doses) and medical conditions (i.e. otosclerosis or abnormal bone growth in the middle ear) are risk factors that have been associated with the onset of tinnitus.
What are the treatment options for tinnitus?
Although there are no cures for tinnitus, there are a number of therapeutic approaches that provide relief and help manage the condition. Audiological solutions include directive counselling, such as Tinnitus Retraining Therapy, in conjunction with sound therapy (i.e. table-top or ear level sound generators and/or hearing aids) to help individuals not only habituate to tinnitus but also improve sound tolerance.
What is Tinnitus Retraining Therapy?
Tinnitus Retraining Therapy (TRT) is a treatment program for tinnitus and hyperacusis using both directive counselling and sound therapy. TRT is used to retrain the subconscious part of the tinnitus sufferer’s brain to ignore the sound of tinnitus. Treatment usually takes 18 to 24 months. If the protocol is followed carefully, some may see improvement by six months. Upon completion of the program, the tinnitus should no longer be bothersome, but if listened for, it will be heard. Continuity of care is essential for achieving results.
What are sound conditioners?
Many tinnitus sufferers find that head and ear noises are not as disruptive in the presence of some pleasing or neutral external sound. Sound conditioners create a variety of soothing sounds that can offer relief, particularly when you are struggling to fall asleep. Consult with your audiologist to find out what might be right for you.